CRANIAL
NERVE III PALSY
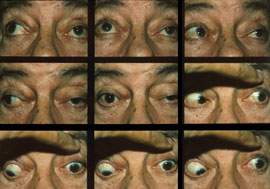
Third nerve palsy
results from damage to the oculomotor nerve anywhere
in its course from the nucleus in the dorsal mesencephalon,
its fascicles in the brainstem parenchyma, the nerve
root in subarachnoid space, or in the cavernous sinus
or posterior orbit. Damage to the third nerve nucleus
results in an ipsilateral third nerve palsy with contralateral
superior rectus under action and bilateral ptosis.
Damage to the third nerve fascicles results in an
ipsilateral third nerve palsy with contralateral hemiparesis
(Weber's syndrome), contralateral intention tremor
(Benedikt's syndrome), or ipsilateral cerebellar ataxia
(Nothnagel's syndrome). Vascular infarct, metastatic
disease and demyelinization are the common causes
of brainstem involvement. Damage to the third nerve
within the subarachnoid space produces an isolated
third nerve palsy. The main causes are compression
of the nerve by an expanding aneurysm of the posterior
communicating artery or the basilar artery, and ischemic
vasculopathy. There will always be pain in aneurysmal
compression and pupillary involvement is typical,
though there have been infrequent cases of aneurysmal
compression that did not initially affect pupillary
function. In ischemic vascular nerve third palsies,
pain is frequent and the pupil is typically normal
and reactive. Damage to the third nerve in the cavernous
sinus, superior orbital fissure, or posterior orbit
is unlikely to present as third nerve palsy due to
the confluence of other structures in these areas.
Cavernous sinus involvement may also include pareses
of cranial nerves IV, VI and V-1, and an ipsilateral
Horner's syndrome. The most common causes of damage
in these areas include metastatic disease, inflammation,
herpes zoster, carotid artery aneurysm, pituitary
adenoma and apoplexy, and sphenoid wing meningioma.
MANAGEMENT
In complicated third nerve palsies where other
neural structures are involved, have the patient undergo
an MRI. In isolated third nerve palsies with no pupillary
involvement where the patient is over 50, MRI scanning,
an ischemic vascular evaluation, and daily pupil evaluation
is indicated.
CRANIAL
NERVE IV PALSY
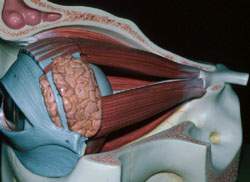
The fourth cranial nerve nucleus is located in the
dorsal mesencephalon. From here, the nerve fibers
then decussate and exit the brain stem dorsally into
the subarachnoid space. The nerve then courses around
the brain to enter the cavernous sinus, superior orbital
fissure, orbit, and innervate the superior oblique
muscle. Damage to the fourth nerve nucleus or its
fascicles within the brain stem will give a contralateral
fourth nerve palsy, along with the associated signs
of light-near dissociated pupils, retraction nystagmus,
up-gaze palsy, Horner's syndrome, and/or internuclear
ophthalmoplegia. Bilateral fourth nerve palsies are
possible as well. The main causes of damage to the
fourth nerve in this area are hemorrhage, infarction,
trauma, hydrocephalus and demyelinization. The fourth
nerve is especially prone to trauma as it exits the
brain stem and courses through the subarachnoid space.
In contrast to third nerve palsies within subarachnoid
space, fourth nerve palsies are rarely due to aneurysm.
The most common causes of damage to the fourth nerve
in this region are trauma and ischemic vasculopathy.
The most likely result from damage within subarachnoid
space is an isolated fourth nerve palsy. Due to the
large number of other neural structures that accompany
the fourth nerve as it travels through the cavernous
sinus and superior orbital fissure, it is unlikely
that the patient will exhibit an isolated fourth nerve
palsy due to damage within these areas. More likely,
there will be an associated palsy of cranial nerves
III and VI. Common causes of damage to the fourth
nerve in these areas are herpes zoster, inflammation
of the cavernous sinus or posterior orbit, meningioma,
metastatic disease, pituitary adenoma, and carotid
cavernous fistula. Trauma to the head or orbit can
cause damage to the trochlea, resulting in superior
oblique muscle dysfunction.
MANAGEMENT
A fourth nerve palsy often presents suddenly, but
may additionally result from decompensation of a longstanding
palsy. In order to differentiate these two types of
palsies, examine old photographs of the patient. A
patient with a decompensated longstanding palsy will
present with a compensatory head tilt in old photos.
Further, patients with decompensated longstanding
fourth nerve palsies will have an exaggerated vertical
fusional ability. Longstanding fourth nerve palsies
typically are benign and no further management is
necessary. In the case of complicated fourth nerve
palsies, (i.e., those that present with other concurrent
neurological dysfunction), the patient should undergo
neuroradiological studies dictated by the accompanying
signs and symptoms. In the case of isolated fourth
nerve palsies caused by recent trauma, the patient
should undergo an MRI or CT scan of the head to dismiss
the possibility of a concurrent subarachnoid hemorrhage.
If the fourth nerve palsy is not associated with recent
trauma, investigate for a history of past trauma.
If the fourth nerve palsy is due to previous trauma
and has recently decompensated, you can manage the
diplopia with vertical prisms. If the patient is elderly
and has a fourth nerve palsy of recent origin, perform
an ischemic vascular evaluation to search for diabetes
and hypertension. If the palsy is caused by vascular
infarct, it will spontaneously resolve over a period
of three to six months and the patient will not require
further management beyond periodic observation and
either temporary occlusion or press-on prism therapy.
CRANIAL
NERVE VI PALSY
Cranial nerve VI arises in the pons, in close association
with the facial nerve and paramedian pontine reticular
formation (PPRF). Due to this arrangement, damage
to the sixth nerve within the brain stem will produce
a sixth nerve palsy as well as a facial nerve palsy
or an internuclear ophthalmoplegia. Associated findings
may also include leg paralysis with sixth nerve palsy
(Raymond's syndrome), or leg paralysis, facial paralysis
and sixth nerve palsy (Millard-Gubler syndrome). These
additional findings identify the location of damage
as the pons, where ischemic infarct, tumor and demyelinization
are the common causes. The sixth nerve travels through
the subarachnoid space where it ascends the clivus
and enters the cavernous sinus. Within the subarachnoid
space, the sixth nerve may be stretched against the
clivus as the brain stem herniates through the foramen
magnum due to increased intracranial pressure. This
will give a bilateral sixth nerve palsy (which is
often intermittent) and papilledema. As the sixth
nerve passes over the petrous apex of the temporal
bone, damage here can result in a sixth nerve palsy,
facial pain and hearing loss. This occurs due to inflammation
of the temporal bone (Gradenigo's syndrome) or nasopharyngeal
carcinoma. Within the cavernous sinus, the sixth nerve
is joined by the oculosympathetic nerves, and cranial
nerves III, IV and V-1. Damage here will yield a sixth
nerve palsy and Horner's syndrome, as well as a concurrent
CN III and IV palsy. The etiology may be aneurysm,
meningioma, pituitary adenoma, inflammation, or fistula.
The sixth nerve is also vulnerable to ischemic infarct
from diabetes and hypertension; this remains a prime
cause of isolated sixth nerve palsy.
MANAGEMENT
A sixth nerve palsy combined with any of the above
mentioned neurological signs indicates a need for
MRI of the appropriate area. In children, sixth nerve
palsy often occurs from a presumed viral cause and
has an excellent prognosis. However, if the palsy
does not recover, or worsens over several weeks, the
child should be examined for a pontine glioma. In
the adult under 50 years, obtain MRI studies of the
brain. Adult over 50 with an isolated sixth nerve
palsy require a workup for ischemic vascular diseases
such as diabetes and hypertension. If the patient
is over the age of 65 years, order an erythrocyte
sedimentation rate (ESR) to rule out giant cell arteritis.
If no etiology is discovered on MRI or hematology
studies, monitor the patient monthly for several months
until resolution (or until other signs develop which
would indicate an etiology). The vast majority of
CN VI palsies due to ischemic vasculopathy (or idiopathic
etiology) will resolve without treatment in three
to six months. Fresnel prism correction or unilateral
occlusion will temporarily alleviate the diplopia.
CRANIAL
NERVE VII (FACIAL NERVE) PALSY
The muscles that close the eyes and wrinkle the forehead
are bilaterally innervated. A unilateral lesion in
the cortex or supranuclear pathway spares eyelid closure
and forehead wrinkling but results in contralateral
paralysis of the lower face. Since the area of the
cortex associated with facial muscle function lies
near the motor representation of the hand and tongue,
weakness of the thumb, fingers and tongue ipsilateral
to the facial palsy is not uncommon. The facial nucleus
contains four separate cell groups that innervate
specific muscle groups. Lesions of the fibers of the
superior salivatory and lacrimal nuclei (parasympathetic
preganglionic fibers supplying the sublingual, submandibular
and lacrimal glands) include temporal bone fractures
and infections, schwannomas, neuromas (cerebellopontine
angle tumors) and vascular compression, producing
deficits in hearing, balance, tear production and
salivatory flow. Lesions that involve the ganglion
include geniculate ganglionitis (Ramsey-Hunt syndrome:
zoster oticus). Lesions such as acoustic neuroma that
also involve cranial nerve VIII can impair hearing,
facial nerve function and produce corneal hypoesthesia
(CN V). Lesions of the zygomatic and lacrimal nerves
impair reflex tear secretion. Middle cranial fossa
disease is indicated when defective tear production
accompanies CN V (muscles of mastication) or CN VI
palsy. Lesions of the facial nerve disable the ability
to dampen sound, producing hyperacusis. Lesions to
sensory afferent fibers that transmit taste (fibers
that also innervate the salivary glands) cause an
interruption in salivatory flow and an inability to
sense taste from the anterior two-thirds of the tongue.
The portion of the facial nerve that contains the
motor fibers that innervate the muscles of facial
expression exits the stylomastoid foramen and enters
the substance of the parotid gland before distribution.
Therefore, investigate lesions of the parotid gland
also as part of the work up. Lesions that occur within
the cortical, extrapyramidal or brainstem levels are
known as central lesions. Lesions outside the brain
are referred to as peripheral. The common causes of
peripheral CN VII palsy include cerebellopontine angle
tumor (7 percent), trauma (21 percent), otitis media,
herpes zoster oticus (Ramsey-Hunt syndrome), Lyme
disease, sarcoidosis, parotid neoplasm, syphilis,
diabetes mellitus, pregnancy and HIV.
MANAGEMENT
First obtain a complete history. Perform a cursory
evaluation of the 12 cranial nerves as well as a comprehensive
ocular examination with dilated fundus and optic nerve
evaluation. Pay close attention to the affected eyelid's
posture, corneal wetting (tear break up time), blink
posture, tear quality (sodium fluorescein staining)
and tear quantity (Schirmer tear testing). In cases
where diagnosis is questionable, ask the patient to
close both eyes while you try to open the lid. If
one lid is significantly easier to open than the other,
suspect CN VII palsy. You can manage exposure keratopathy
with ocular lubricating drops and ointments. Moisture
chamber patches (e.g. Guibora eye patch) or eyelid
taping are also possible solutions. Moisture chamber
shields can be attached to spectacle temples to create
a moist ocular environment and lessen tear evaporation.
Since idiopathic facial nerve palsy is a diagnosis
of exclusion, order laboratory testing (Lyme titer,
rheumatoid factor, erythrocyte sedimentation rate,
antinuclear antibody, echocardiogram, fluorescent
treponemal antibody absorption test, HIV titer, chest
X-ray), lumbar puncture (in patients with suspected
neoplasm), CT and MRI and/or appropriate referrals
(otolaryngology, neurology, neurosurgery).